De Quervain’s Tenosynovitis is a painful condition which affects the thumb muscles (Abductor Pollicis Longus and extensor Pollicis Brevis).
Commonly seen in females who are in the post-natal phase, it is caused by a rapid increase in load on the thumb muscles and tendons. This over-load is usually caused from repetitive feeding positions, lifting and holding of an new infant. It can also commonly occur in golfers.
Symptoms will include swelling and local tenderness over the tendons. It can also be a sudden sharp feeling, which is not ideal when holding a young child!
Diagnosis
It is diagnosed by conducting a simple test called the Finkelstein test. The tests involves bending your thumb across the palm of you hand and then bending your fingers over the thumb. The wrist is then bent toward your little finger. If this reproduces the same pain you experience, it is likely De Quervains syndrome.
A physiotherapist will also conduct some tests on the joints around the thumb and wrist to exclude them as a source of the symptoms.
Treatment
Successful treatment techniques include splinting/bracing of the wrist to off-load the thumb tendons, and then progressive weaning from the brace to reintroduce load in a monitored way.
Gradual strengthening of the tendon is highly important as increasing the tendons tolerance to load is the fundamental component of rehab. As with any tendon strength program, load needs to be slowly introduced as a sudden increase in strength exercises can easily overload and aggravate the tendon! If bracing is left on for too long the tendon will become weaker and hence when you remove the brace the pain will come back.
If you start treatment early, your symptoms should improve over the next 4-6 weeks. If your symptoms start during or after pregnancy your symptoms are likely to resolve once breast feeding has stopped.
Despite common belief, a corticosteroid injection is not the first line treatment. An injection should only be considered if bracing and physiotherapy has failed over a 4-6 week period.
TOP TIPS:
ICE for pain relief
BRACE to off-load the tendon
STRENGTH to increase the tendons tolerance to load (likely the reason the thumb was sore in the first place).
CORTISONE injection only after 6 weeks if the above fails.
If you have any questions or if you think you may have De Quervain’s then please do not hesitate to get in touch with us here.
Ankle sprains or “inversion injuries” are one of the most common injuries experienced by recreational and elite athletes, accounting for approximately 10-30% of all sports related injuries across a number of sports including soccer, netball, basketball and rugby.
How does an ankle sprain occur?
An ankle sprain generally occurs when the ankle “rolls” inwards, as a result of uneven playing surfaces, landing awkwardly following a jump or changing direction. The ligaments, tendons and joint capsule on the outside of the ankle are stretched beyond their capacity, causing injury.
Anatomy
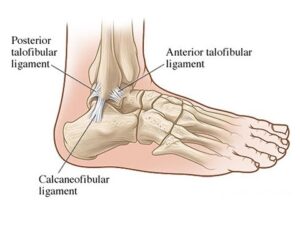
Approximately 85% of all ankle sprains occur to the lateral ligament complex which is comprised of the anterior talofibular ligament (ATFL), joint capsule, calcaneofibular ligament (CFL) and the posterior talofibular ligament (PTFL) (See picture below).
The ATFL is involved in the majority of lateral ankle sprains; the CFL in approximately 40% and the PTFL in less than 10% of all injuries.
How do I know if I have rolled or sprained my ankle?
Following an acute ankle sprain, pain is generally felt on the outside of your ankle which is often accompanied by immediate swelling, which can be localised to the ankle or present in the foot and toes depending on the severity of your injury. There is also often bruising or skin discolouration on the inside and/or outside of the foot, however this has not been shown to determine the severity of your injury or indicative of a fracture to one of the bones in your ankle or foot.
How do I know if it’s more serious than just a sprain?
The Ottawa ankle rules are accurate guidelines that are used by doctors and physiotherapists to determine whether or not an x-ray should be obtained following an ankle sprain. These guidelines include:
Younger than 16 OR older than 55 years of age (as their bones are softer)
Bone tenderness of the medial or lateral malleolus, navicular or base of the 5th metatarsal (pictured below)
Unable to weight bear immediately after the injury for 4 steps
Less than 15% of all ankle sprains result in a fracture, so if you suspect you may have suffered one see your doctor or physiotherapist for a thorough assessment and referral for an x-ray of your ankle or foot.
What’s the best early management of my ankle sprain?
Right after an ankle injury, the most important thing you can do is try to reduce your pain and inflammation as fast as possible. This is best achieved by following the PRICER protocol, which includes:
Protection – Avoid activities that may cause further damage or pain
Relative rest – Avoid activities that cause pain to the area but don’t avoid moving the ankle as this will slow the recovery process (let pain be your guide)
Ice – Apply an ice pack for 20 minutes every 1-2 hours for the first 72 hours
Compression – Apply a compression bandage to minimise and control swelling
Elevation – Elevate the ankle above the level of your heart
Referral – Medical assistance should be sought as soon as possible to determine the extent of the injury and develop a rehabilitation plan for full recovery return to sport.
Medications such as Panadol may also be necessary to control pain, however research suggests that anti-inflammatory medications should not be used within the first 72 hours as they can impact the normal inflammatory process which is essential for healing, we want to control the swelling, not stop it completely!
What will my rehabilitation consist of?
Adequate rehabilitation following an ankle sprain is very important. Recent studies have shown that not only do 30% of individuals who suffer ankle sprains end up with persistent symptoms such as pain and swelling but 20% also have recurrent episodes of ankle sprains, so rehabilitation is vital to not only reduce symptoms and return you to full function but also to prevent re-occurrence of future ankle sprains.
Physiotherapy will include a thorough assessment of your ankle and foot to determine what structures have been injured. Treatment can start on day 1 and will depend on the type of injury you have sustained but will normally include:
Management of pain and swelling (strapping/bracing)
Hands-on manual therapy in order to restore normal joint movement
An individually tailored rehabilitation program to restore flexibility, strength and proprioception (balance) as well as prevent future injuries
Sports specific exercises to ensure safe return to sport
Advice on how maintain your fitness throughout the rehabilitation process
How long will it take to recover?
Every ankle sprain is different and the recovery time and return to sport will vary depending on individual factors such as effective early management, the extent of the injury, previous history of injury and underlying flexibility, strength and proprioception issues. However, as a rough guide mild ankle sprains with minimal fibre damage generally take 2-4 weeks, moderate ankle sprains 4-6 weeks and severe ankle sprains with complete ligament ruptures and/or fractures 6-12 weeks for full recovery.
For any further information, please do not hesitate to contact us at Clinical Physio, St Ives clinicalphysiostives.com.au
Medial Tibial Stress Syndrome (MTSS) or “shin splints” is one of the most commonly reported lower limb injuries by competitive and recreational athletes. Recent research has shown that shin splints affects approximately 20% of the running population, with the majority of sufferer’s partaking in long distance training/competition.
What causes the pain?
Currently, there is two widely accepted theories on the cause of shin splints:
The bony bending/bowing theory
The traction theory
The bony bending theory suggests that during running, the Tibia (shin bone) bends due to the stress placed upon it. This bending causes small amounts of strain in the bone that enables it to adapt and get stronger (a good thing!!). When this strain exceeds the adaption process the shin bone becomes overloaded (a bad thing!), subsequently leading to injury and pain.
The traction theory states that shins splints is caused by the continual contraction of the muscles (Soleus, Flexor Digitorum Longus & Tibialis Posterior) that attach to the inner border of the shin. As these muscles contract during running, they place a traction stress on the shin bone, which results in inflammation at their attachment onto the bone, causing pain.
Am I at risk?
Current research has identified several risk factors leading to an increased likelihood of developing shin splints. These include:
A previous history of shin splints
Prior orthotic use
High Body Mass Index (BMI)
Female gender
Decreased running experience
Decreased running cadence (step rate)
Excessive pronation
Over striding
Crossover running style
Increased vertical oscillation (ground clearance)
Forefoot running
How do I know if I have shin splints?
To diagnose shin splints accurately, two symptoms must be present:
Exercise induced pain along the distal 2/3 of the medial Tibial border
Recognisable pain produced by pressing the medial Tibial border, which spans a distance of 5cm or more.
If you are experiencing symptoms not typical of shin splints such as cramping, pain spanning less than 5cm, burning pain, numbness or pins and needles, you should seek a thorough assessment by a physiotherapist to properly diagnose and treat your condition.
Treatment – Technique Technique Technique!!!
Arguably one of the biggest contributors to the development of shin splints in a runner is their running technique, particularly their lower limb mechanics. One of the quickest ways to reduce shin splints related pain is to address the technical aspects of running that can contribute to increased stress across the Tibia and associated musculature. What you should focus on is:
Cadence – Normal cadence should be between 165-185steps/min. Decreased Cadence causes increased ground contact time resulting in prolonged pronation and excessive tibial torsion stress.
Over striding – Excessive stride length results in poor tibia positioning upon heel strike, increasing Soleal traction and reducing force absorption ability.
Cross Over Gait– Landing across the midline of the body causes excessive tibial torsion and pronation, reducing proper force attenuation.
Vertical Oscillation– Increased vertical oscillation during running increases Tibial impact forces and often results in a loud foot strike.
How do I improve my technique?
Increase your cadence!! – This is by far the biggest bang for your buck. Increasing your cadence by approximately 10%:
Reduces lower limb impact forces by 20%
Reduces vertical oscillation
Reduces ground contact time
Reduces stride length
The best way to achieve an increase in your cadence is by using GPS watches, phone applications or by simply running on a treadmill.
Eliminate a crossover running style – On a track, run straddling a line across 2 lanes or alternatively, try and maintain a space between your knees with every stride.
How to beat shin splints using strength
Strength exercises for shin splints should aim to improve the localised muscular capacity of the calf complex as well as the bone load capacity of the Tibia. This is best addressed with weight bearing functional exercises that mimic running postures.
One of the most important and often forgotten muscles of the calf complex is the Soleus. The soleus muscle is vital for absorbing excessive loads placed on the Tibia during running by minimising excessive pronation as well as resisting the bending forces experienced by the Tibia due to ground impact.
The best Soleus exercise that runners can do is the Bent Knee calf raise (pictured above). To perform the exercise correctly:
Bend your knee as far forward as possible, keeping your foot flat on the floor
Keeping your knee bent, raise yourself up onto your toes
Lower your heel back to the ground
Perform 3 sets of 15 repetitions in a slow and controlled manner.
As always, if you are having problems, please do not hesitate to contact one of our experienced physiotherapists.
Hip bursitis or “trochanteric bursitis” has historically been used to describe pain on the outside of the hip. Recent research has found that only 20% of individuals presenting with pain on the outside of the hip have bursal thickening on ultrasound (Grimaldi & Fearon, 2015).
Whereas changes in the gluteus Medius and gluteus minimums tendons are much more commonly observed on scans. Bursal changes are now known to be an incidental finding, with bursal swelling occurring as a protective mechanism to reduce damage to the tendons. As such, hip bursitis is now referred to as gluteal tendinopathy and is recognised as the primary cause of pain and tenderness on the outside of the hip that may extend down the outside of the thigh.
Who gets it?
Gluteal tendinopathy affects 10-25% of the population and is experienced by one in four women aged over 50 years (Mellor et al., 2018).
Females tend to be at the highest risk of developing the condition, with a 4:1 ratio compared to males. Clinically, it is also commonly seen in runners and those with prior hip injuries or hip surgery.
Why does it occur?
Gluteal tendinopathy occurs as a result of repetitive compression of the tendons against the greater trochanter (the bone you can feel on the outside of your hip). Repetitive loading of the gluteus Medius and gluteus minimums can overload these tendons, as they are unable to adequately withstand the demands placed upon them.
Continually applying excessive load to the tendons progressively worsens the condition, as small micro tears occur in the tendons causing inflammation, pain and dysfunction.
Typical activities causing compression and irritation of the gluteal tendons include running, walking upstairs, crossing the legs or sleeping on the affected side at night.
How do I know if I’ve got Gluteal Tendinopathy?
Gluteal tendinopathy is characterised by pain on the outside of the hip and outer thigh. Typically people with gluteal tendinopathy experience at least one or more of the following symptoms –
Pain sitting with crossed legs
Pain going from sitting to standing
Pain with prolonged standing or pain standing on the affected leg
Pain going up stairs
Pain with walking/running
Difficulty lying on the sore side at night
Hip Bursitis causes and exercises
How did I get it?
Gluteal tendinopathy can develop due to a number of contributing factors such as –
Muscular weakness (glutes)
Muscular tightness
Commencing a new activity e.g. gym, vigorous walking
A recent increase in training load
Biomechanical abnormalities e.g. over striding
How do I fix it?
The first stage in managing gluteal tendinopathy is to control pain by minimising the compression on the greater trochanter and managing load on the tendons. Depending on the severity of the condition, this may involve temporarily limiting aggravating activities such as running and stairs, to enable healing and allow time for symptoms to settle.
Once symptoms are better controlled, overwhelming research evidence supports commencing strength training of the gluteal muscles. Studies have shown significant strength deficits of the hip abductors (glute med & glute min) in individuals with gluteal tendinopathy, with those who had gluteal tendinopathy being 32% weaker on the painful side and 23% weaker on the non-painful side (Allison et al., 2016).
Tailored strength programs targeting these muscles can effectively improve pain and restore function, by increasing the capacity of the tendons to cope with the demands of everyday activities.
The good news is the majority of individuals who undergo a progressive strengthening program will recover from gluteal tendinopathy within 3 months.
Two Best Exercises for Hip Pain
What to avoid?
To prevent further irritation, it is necessary to reduce compression of the tendons. This can be achieved through the following management strategies –
Reducing time with legs crossed
Not ‘hanging’ on one hip in standing
Reducing stride length when walking
Using a rail to climb stairs and placing feet wider when walking up stairs
Avoiding stretching of the glutes
Placing a pillow between the knees when sleeping on the side
Should I get an Injection for my hip bursitis?
Corticosteroid injections have traditionally been used to treat help manage pain in gluteal tendinopathy, however recent evidence suggests they may actually prolong recovery.
A 2018 Australian study comparing individuals with gluteal tendinopathy who received corticosteroid injections to those who underwent strengthening exercise, found exercise to be superior both in the short and longer-term. While both groups had similar reductions in pain at both 8 and 52 week follow-up, the exercise group reported a significantly better global improvement in function than corticosteroid injection use (Mellor et al., 2018). Thus, exercise is considered the current cornerstone treatment for non-surgical management of gluteal tendinopathy.
Take home messages:
Gluteal tendinopathy (previously hip bursitis) is an overload problem related to activity
It is reversible and can be improved with non-surgical management
Corticosteroid injections may prolong recovery
STRENGTH training is best!
References:
Allison, K., Vicenzino, B., Wrigley, T. V., Grimaldi, A., Hodges, P. W., & Bennell, K. L. (2016). Hip Abductor Muscle Weakness in Individuals with Gluteal Tendinopathy. Med Sci Sports Exerc, 48(3), 346-352. doi:10.1249/MSS.0000000000000781
Grimaldi, A., & Fearon, A. (2015). Gluteal Tendinopathy: Integrating Pathomechanics and Clinical Features in Its Management. J Orthop Sports Phys Ther, 45(11), 910-922. doi:10.2519/jospt.2015.5829
Mellor, R., Bennell, K., Grimaldi, A., Nicolson, P., Kasza, J., Hodges, P., . . . Vicenzino, B. (2018). Education plus exercise versus corticosteroid injection use versus a wait and see approach on global outcome and pain from gluteal tendinopathy: prospective, single blinded, randomised clinical trial. Br J Sports Med, 52(22), 1464-1472. doi:10.1136/bjsports-2018-k1662rep
Tennis elbow is defined as a cause of pain and tenderness in the outer part of the elbow (lateral epicondyle) where the tendons of the forearm muscles attach.
It is an overuse injury from repetitive or forceful/explosive movements involving eccentric motion and/or in which the wrist frequently deviates from a neutral position. This can be from training errors, inadequate equipment or poor environmental conditions.
Who can get Tennis Elbow?
Tennis elbow can affect anyone, however is more common in people between 30 and 60 years of age. It appears to be more severe and of longer duration in females. The most commonly affected arm is the dominant arm. It is commonly seen in office workers (repetitive typing) or manual labour workers (carpenters etc).
Signs and Symptoms of Tennis Elbow?
Pain and tenderness over the elbow bone (lateral epicondyle)
Pain with gripping, twisting, lifting.
Some cases may have nerve involvement – nerve pain and neck range of motion restrictions.
Do I need an X-ray or MRI?
A diagnosis can be made based on the history of the condition and a physical examination. X-rays may be used to help rule out other causes of elbow pain, such as arthritis. An ultrasound or magnetic resonance imaging (MRI) scan will show the degenerative changes or small tears in the tendon, but is rarely required.
Tennis Elbow Treatment
Evidence tells us that strength exercises are the most effective way of treating tennis elbow, with adjuncts of manual therapy (lateral elbow glides and C5 glides if radial nerve involvement. (L.Bisset et al 2015, Cleland et al 2013).
Strength exercises can not only help settle the pain, but also reduce the risk of the pain returning.
Each patient should be treated based on the history and the findings. Common treatments include:
Load management: – Reducing or stopping the aggravating activity for a short period- Progressive loading and strengthening to improve load capacity
Ergonomic advice (for example, the amount of time spent out of neutral wrist position is strongly associated with tennis elbow)
Correction of biomechanics if required for return to sport.
Tips & Tricks:
Avoid the aggravating activities or positions that bring on your pain
Carry things with your palm up
Carry things close to the body
Load the tendon with exercises, but reduce manual labour
There should be no pain when performing exercises
Patients can also be reassured that some cases will improve without intervention and just information regarding modification of aggravating activities, ergonomic advice and reassurance that their condition will eventually settle.
Cortisone injections for tennis elbow… do they work?
Corticosteroid injections are NOT recommended. In a study by Vicenzino et al 2006, 198 participants got assigned to three groups (physiotherapy interventions, corticosteroid injections and ‘the wait and see approach’). The corticosteroid group had most reported recurrences at 72%.
Is there any evidence for any other treatment options?
Chiropractic manipulation
Can provide short term pain relief, however has no effect on long term outcome.
Bracing/taping
There is conflicting evidence for the effectiveness of bracing/taping compared with placebo or no treatment.
Acupuncture/dry needling
Conflicting evidence, but may be more effective than placebo and ultrasound at relieving pain and improving self-assessed treatment benefit in the short term.
Laser therapy
May be beneficial in short term compared with placebo, likely no difference between laser and other active interventions in the short or long term.
Ultrasound
No more effective than placebo for pain relief or self-perceived global improvement in short term.
Shock wave therapy
Little or no benefit in reducing pain or improving function.
Platelet rich plasma injections
No benefit.
If you have any questions, or would like our help, please do not hesitate to get in touch at clinicalphysiostives.com.au
References:
1) Physiotherapy management of lateral epicondylalgia – Bisset, Vicenzino (2015)
•Hypoalgesic and sympathoexcitatory effects of mobilization with movement for lateral epicondylalgia – Paungmali, O’Leary, Souvlis, Vicenzino (2003)
2) Specific manipulative therapy treatment for chronic lateral epicondylalgia produces uniquely characteristic hypoalgesia – Vicenzino, Paungmali, Buratowski, Wright (2001)
•Manipulation of the wrist for management of lateral epicondylitis: A randomized pilot study – Struijs, Damen, Bakker, Blankevoort, Assendelft, Van Dijk (2003)
3) Incorporation of Manual Therapy Directed at the Cervicothoracic Spine in Patients with Lateral Epicondylalgia: A Pilot Clinical Trial – Cleland, Flynn, Palmer (2013)
4) A randomized controlled trial of eccentric vs. concentric graded exercise in chronic tennis elbow (lateral elbow tendinopathy) – Peterson, Butler, Eriksson, Svardsudd (2014)
5) Mobilisation with movement and exercise, corticosteroid injection, or wait and see for tennis elbow: randomised trial – Bisset, Beller, Jull, Brooks, Darnell, Vicenzino (2006)
6) Addition of isolated wrist extensor eccentric exercise to standard treatment for chronic lateral epicondylosis: A prospective randomized trial – Tyler, Thomas, Nicholas, Malachy, McHugh (2010)
7) Is tendon pathology a continuum? A pathology model to explain the clinical presentation of load-induced tendinopathy – Cook & Purdam (2009)