The latest update on Physio and Headache management.
Back in 2016 Andrew wrote a great blog article on the role of physio in assessing and treating headache. Well with the headache that was 2020 behind us, I thought I would start the new year with the latest information and research on how physio can help that pain in your head.
What are the common headaches that physios see?
There are 3 common headache types that physios generally see:
Cervicogenic
Tension
Migraine
Cervicogenic (headache coming from the neck) are generally one sided, will start with neck pain and progress to the head. You may also find neck stiffness and checking your blind spot whilst driving to be difficult.
A cervicogenic headache is essentially referred pain from the neck that, due to a miscommunication of the nerves that supply the head and neck, the pain is perceived in the head, rather than the true source in the neck.
The pathophysiological basis for the referred pain is a “convergence” of nerves. To try to put it simply, the nerves that supply the head come into close proximity to the nerves that supply the neck. As the nerves from the neck make there way into the brain to communicate the message of neck dysfunction, they “converge” with the nerves that are carrying messages from the head. The end result is that the brain thinks the message is coming from the head, rather than the neck.
Tension headaches feel like you’re wearing a swimming cap that’s a little too tight! It will feel like a tightening pain around your whole head. You may also have neck pain related to this headache.
Migraine headaches are commonly one sided and intensely painful. Most people say they either feel sick in the stomach or don’t like bright lights/sound. Some people will also get an aura (seeing bright lights and colour) before their pain comes on. Neck pain can occur with Migraine however is less common.
Signs that your headache may be coming from you neck
1) Neck stiffness
2) Your headache changes when your turn your head i.e may be worse when trying to turn your head in one direction
3) Tenderness of the upper cervical region. It may be sore and sensitive to push on the muscles and joints at the top of your neck.
Does posture affect headaches?
How many times have you heard or thought ‘Wow I’ve got bad posture’. Well, all your worrying may be for nothing. There has been some great research into posture and headache, which has found that people with headaches have many different postures.
There was not one posture that made people more likely to suffer from headache.
Additionally, other factors such as stress, lack of sleep and reduced physical activity have a much larger effect on developing headaches.
So, is there a good posture? The best evidence we have suggests that changing posture, rather than having one specific posture, is the best approach to take.
Can physio help your headache?
Short answer…yes! There has been lots of research into physio and headache, which shows that we can help reduce the intensity, frequency and duration of headache.
How do we do this?
Hands on treatment of the joints and muscles in the neck can be very helpful to reduce headache pain and stiffness. However, the effects of these treatments don’t always treat the common, underlying muscle problem.
A study on 52 women in 2019 in the Journal of Orthopaedic & Sports Physical Therapy found that “Women with migraine demonstrated decreased neck flexor and extensor muscle endurance compared to women without migraine.”
We have found that improving the endurance of the neck muscles helps to improve the ability to do simple things like…reading, texting or even just sitting/standing long periods.
Headaches affect up to 50% of the population at some stage in their lives. At least 20% of all headaches and migraines can be attributed to the neck and some studies show this number may be significantly higher.
What is a cervicogenic headache?
A cervicogenic headache is essentially referred pain from the neck that, due to a miscommunication of the nerves that supply the head and neck, the pain is perceived in the head, rather than the true source in the neck. The pathophysiological basis for the referred pain isa “convergence” of nerves. To try to put it simply, the nerves that supply the head come into close proximity to the nerves that supply the neck. As the nerves from the neck make there way into the brain to communicate the message of neck dysfunction, they “converge” with the nerves that are carrying messages from the head and thus the end result is that the brain thinks the message is coming from the head, rather than the neck.
What can a physiotherapist do?
Our jobs, as physiotherapists, are to:
correctly identify headaches that are caused by a neck (cervical) dysfunction;
correctly identify what type of dysfunction it is and;
treat the underlying cause of the dysfunction to promote good, long-term outcomes.
How can we correctly identify a cervicogenic headache?
It can take 60-90mins to thoroughly assess and diagnose a headache as the symptoms and physical findings are complex and differ from patient to patient. The first step is to look at the history and symptoms. These typically include:
Gradual onset of symptoms (won’t come on sharply or suddenly)
Episodes are similar to each other i.e. symptoms do not worsen episode to episode
Location
Will generally by one-sided and will not shift sides within the same episode
Can be one of, or a combination of, neck, occipital (at the back), parietal (at the side) or orbital (around and behind the eye)
Can last anywhere from 1 hour to 1 week
Feels non-throbbing
Aggravated by neck movements or sustained postures
Other symptoms can include nausea, vomiting, visual disturbances and sensitivity to light and sound
If your symptoms fit the above criteria then the next step is to conduct a thorough musculoskeletal exam. This includes, but is not limited to,
Posture assessment
Ergonomic assessment if work seems to be an aggravating factor
Neck range of motion and strength testing
Shoulder and scapular range of motion
Thoracic range of motion
Palpation assessment, particularly looking for stiffness, position, tenderness and/or referred pain from the top 3 cervical joints
Cervical flexion rotation test (CFRT)
This test has been found to have good reliability in diagnosing cervicogenic headache (Hall et al, 2008)
If your symptoms still fit the criteria for a cervicogenic headache, we can then move on to addressing the findings from the physical assessment.
Treatment
Treatment will depend on the findings from the subjective history as well as the physical exam and can include, but are not limited to,
Neck and thoracic spine mobilisations
Thoracic manipulations
Ergonomic adjustments to workstation
Strengthening exercises for the deep neck stabilisers, neck and thoracic extensors and upper trapezius/shoulder girdle muscles.
Sustained Natural Apophyseal glides (SNAGs) for the C0- or C1-2segments (see video)
2 recent systematic reviews released in The European Spine Journal (Varatharajan et al, 2016) and the Journal of Manual Therapy (Gross et al 2016) both found that exercise combined with mobilisations is an effective treatment option for headache and can also decrease medication intake in the short and long term.
If the above signs and symptoms sound familiar, then please do yourself a favour and book an appointment with an experienced physiotherapist.
Does your jaw click? Do you grind your teeth or wake up in the morning with sore teeth? Does it hurt to open your mouth all the way? Or hurt to chew? These are all signs that there may be an issue with your temporomandibular joint (TMJ).
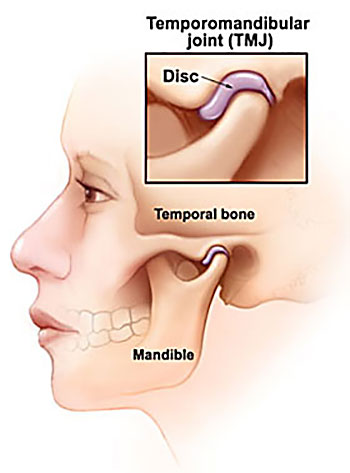
Simple Anatomy
The TMJ is a common, yet poorly understand cause of headache and neck pain. It is actually a fairly simple structure and acts like many other joints in the body with surrounding muscles acting on the joint to produce movement up and down and side to side. It has a small disc inside the joint that allows for smooth movement of the joint. It is this disc translating forwards/backwards that can cause “clicking” when you open and close.
Cause of pain in the TMJ
There are 2 main structures which are sources of pain in the TMJ.
1) The muscles – in particular the large masseter muscle that sits on the outside of the jaw. If you place a finger on the outside of your jaw and clench, you can feel this muscle bulge into your finger. The other muscles are the medial and lateral pterygoid muscles which sit inside the mouth and help to open and close and move the jaw forwards. These muscles can either get tight/overworked (particularly if your stressed) or can also become weak.
A recently published study by Greenbaum et al (2021) found that the muscles of the TMJ are the primary cause of headache from TMJ disorders and 38% patients with muscular TMJ disorders will develop headache.
2) The Joint, including the small disc that sits inside the joint. The joint has 2 main movements. 1 is to “roll” open and closed and the other is movement side to side. The disc helps to cushion the joint when we clench and also aids the lubrication of the joint.
The joint can become painful either due to trauma, developing poor chewing mechanics or, again, if there is some underlying stress/anxiety causing jaw clenching at night. Greenbaum’s conclusions also found that if the primary cause of jaw pain is from the joint, there is almost a 0% chance that you will develop a headache.
How can the TMJ cause a headache?
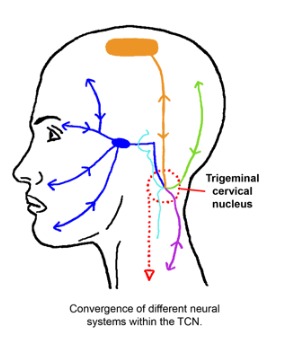
As stated above, the muscles of the TMJ are the primary cause of headache. These muscles can refer into the head due to a phenomena known as “convergence”. This is where the nerves that supply the jaw muscle (in blue in the pic below) converge/communicate via the same nerves that supply the head (in green and orange).
All these nerves share a common central nucleus, almost like a roundabout, where these nerves all meet then go there separate ways again. Our brains can get a little confused as to the source, so we end up experiencing pain in both the jaw and the head.
Treatment
Treatment really depends on what we find during the assessment. For example, in order to assess for muscle weakness or overactivity of the pterygoids we conduct some specific movement and strength tests. If we do find an issue with overactivity, then we may do a muscle release on the pterygoids then reassess your jaw movement again.
The can also be a link between poor posture and TMJ pain. This test to determine if there is a link is quite simple. We place the patient in a “poor posture” position i.e. slumped with head forward and ask them to open and close. We then place the patient in an upright position, with head back and ask them to open and close again. If posture is contributing to the symptoms, the patient will report less pain and also be able to open their jaw further.
If you do have jaw pain, or potentially a headache that you now think might be originating from your jaw, please don’t hesitate to get in touch with us at clinicalphysiostives.com.au
Does your jaw click? Do you grind your teeth or wake up in the morning with sore teeth? Does it hurt to open your mouth all the way? Or hurt to chew? These are all signs that there may be an issue with your temporomandibular joint (TMJ).
Simple Anatomy
The TMJ is a common, yet poorly understand cause of headache and neck pain. It is actually a fairly simple structure and acts like many other joints in the body with surrounding muscles acting on the joint to produce movement up and down and side to side. It has a small disc inside the joint that allows for smooth movement of the joint. It is this disc translating forwards/backwards that can cause “clicking” when you open and close.
Cause of pain in the TMJ
There are 2 main structures which are sources of pain in the TMJ.
1) The muscles – in particular the large masseter muscle that sits on the outside of the jaw. If you place a finger on the outside of your jaw and clench, you can feel this muscle bulge into your finger. The other muscles are the medial and lateral pterygoid muscles which sit inside the mouth and help to open and close and move the jaw forwards. These muscles can either get tight/overworked (particularly if your stressed) or can also become weak.
A recently published study by Greenbaum et al (2021) found that the muscles of the TMJ are the primary cause of headache from TMJ disorders and 38% patients with muscular TMJ disorders will develop headache.
2) The Joint, including the small disc that sits inside the joint. The joint has 2 main movements. 1 is to “roll” open and closed and the other is movement side to side. The disc helps to cushion the joint when we clench and also aids the lubrication of the joint.
The joint can become painful either due to trauma, developing poor chewing mechanics or, again, if there is some underlying stress/anxiety causing jaw clenching at night. Greenbaum’s conclusions also found that if the primary cause of jaw pain is from the joint, there is almost a 0% chance that you will develop a headache.
How can the TMJ cause a headache?
As stated above, the muscles of the TMJ are the primary cause of headache. These muscles can refer into the head due to a phenomena known as “convergence”. This is where the nerves that supply the jaw muscle (in blue in the pic below) converge/communicate via the same nerves that supply the head (in green and orange).
All these nerves share a common central nucleus, almost like a roundabout, where these nerves all meet then go there separate ways again. Our brains can get a little confused as to the source, so we end up experiencing pain in both the jaw and the head.
Treatment
Treatment really depends on what we find during the assessment. For example, in order to assess for muscle weakness or overactivity of the pterygoids we conduct some specific movement and strength tests. If we do find an issue with overactivity, then we may do a muscle release on the pterygoids then reassess your jaw movement again.
The can also be a link between poor posture and TMJ pain. This test to determine if there is a link is quite simple. We place the patient in a “poor posture” position i.e. slumped with head forward and ask them to open and close. We then place the patient in an upright position, with head back and ask them to open and close again. If posture is contributing to the symptoms, the patient will report less pain and also be able to open their jaw further.
If you do have jaw pain, or potentially a headache that you now think might be originating from your jaw, please don’t hesitate to get in touch with us at clinicalphysiostives.com.au