Lower back pain is the single most common musculoskeletal complaint in the world. Up to 85% of the population will complain of low back pain at some stage in their lives. It is also the 3rd most common reason people will visit a GP.
Lower back pain can be broken into 2 broad types.
Central Low Back Pain – pain that does not dominate one side and is experienced generally across the entire lower back region.
Unilateral Low Back Pain – pain that is experienced on one side only.
It is this second that we are going to talk about.
Whilst there are other possible causes of unilateral low back pain, the most common cause we see is actually the hip. The reason is that when we load the lower limbs in tasks such as getting out of a chair, walking, running, climbing stairs, this load is transferred from the ankle, through the knee, then to the hip and then finally the lower back. If the hip is not functioning optimally, this load will bypass the hip and be transferred straight into the lower back on the same side.
Because the hip has significant movement in all 3 planes (forwards, backwards, side to side and rotation) it plays a much more complex role than the ankle and knee which move predominantly in 2 and 1 planes respectively. Back pain on one side can also be attributed to the ankle or knee but these are less common causes.
What does the evidence say?
Sadeghisani and colleagues in 2015 conducted a review of all the published literature of hip range of motion and its relationship to low back pain. They concluded that hip range of motion testing, particularly hip internal rotation, should be a standard, routine part of an examination for patients with low back pain.
Eyvazov and colleagues in 2016 conducted a study on 28 patients booked in for a hip replacement found that their concomitant lower back pain was reduced by 50% after their surgery.
A study earlier this year by Prather and colleagues on 101 patients with low back pain found that those with positive hip examination findings (predominantly reduced hip flexion and internal rotation range of motion), had more pain and poorer function compared to those with normal hip findings.
Sorenson and collegues (2016) found that asymetrical performance of hip abduction (moving the leg out to the side) was a significant risk factor for people that get low back pain when standing.
How do we find out if your hip is the problem?
There are 2 parts to the assessment.
Assessment of your lumbar movements in positions that you have reported to be a problem. For example if you get your pain during or after running, then we’ll get you on the treadmill to have a look at what happens around the hip when you run. If you get the pain simply getting out of a chair, then we’ll examine that movement. We will often find that due to reduced hip function, there are abnormal compensatory movements that occur in the lumber spine.
Assessment of hip strength and range of motion on the same side. Often if the pain is related to the hip, there will be deficits in either strength or range of motion or both, on the same side as your pain. Studies show that the 2 most important movements to assess are hip flexion and hip internal rotation.
If you are suffering from lower back pain one one side then don’t be afraid to get in touch with us to have your hip checked out.
Ellison JB, Rose SJ, Sahrmann SA. Patterns of hip rotation range of motion: a comparison between healthy subjects and patients with low back pain. Phys Ther. 1990; 70(9): 537-541.
Chesworth BM, Padfield BJ, Helewa A, et al. A comparison of hip mobility in patients with low back pain and matched healthy subjects. Physiotherapy Canada. 1994; 46: 267-74.
Eyvazov K, Eyvazov B, Basar S, Nasto LA, Kanatli U. Effects of total hip arthroplasty on spinal sagittal alignment and static balance: a prospective study on 28 patients.Spine J. 2016 Nov;25(11):3615-3621. Epub 2016 Jul 15.
Prather H, Cheng A, Steger-May K, Maheshwari V, Van Dillen L. Hip and Lumbar Spine Physical Examination Findings in People Presenting With Low Back Pain, With or Without Lower Extremity Pain.Orthop Sports Phys Ther. 2017 Mar;47(3):163-172. doi: 10.2519/jospt.2017.6567. Epub 2017 Feb 3.
Sorensen CJ, Johnson MB, Norton BJ, Callaghan JP, Van Dillen LR. Asymmetry of lumbopelvic movement patterns during active hip abduction is a risk factor for low back pain development during standing.Mov Sci. 2016 Dec;50:38-46. doi: 10.1016/j.humov.2016.10.003. Epub 2016 Oct 13.
Sadeghisani M, Manshadi FD, Kalantari KK, Rahimi A, Namnik N, Karimi MT, Oskouei AE. Correlation between Hip Rotation Range-of-Motion Impairment and Low Back Pain. A Literature Review.Traumatol Rehabil. 2015 Oct;17(5):455-62. doi: 10.5604/15093492.1186813.
You’re at home, you reach down to pick up your shoes and “bang” you get this sudden, crippling back pain. You call your physio/chiro/osteo/doctor. They assess you and say that you probably have a slipped disc or a disc bulge and that you need an MRI. You go home, jump on the world wide web and are confronted with all sorts of pictures showing discs pushing on nerves. Every website you read says that you may need surgery and you should be avoiding heavy lifting, bending and twisting. Sound familiar?
There are 3 main problems with the above scenario.
1. Scans rarely add value.
Patients symptoms rarely correlate with what we see on their scans . A systematic review by Brinjiki and colleagues in 2014 looked at all the studies published on asymptomatic people i.e. they had no symptoms or history of symptoms. They found that all the studies regularly reported disc problems in pain free subjects.
30% of all 20yr olds had a disc bulge and no pain. This percentage increased with age, with over 60% of 50yr olds having a disc bulge, and these are people who had no symptoms whatsoever. We also regularly find that patients with acute, crippling low back pain have no evidence of acute tissue damage on MRI.
A study in 2015 (Fritz and colleagues) also found that back pain patients who had an MRI or CT scan spent up to $5,000 more on rehabilitation compared to those who didn’t . The reason for this is multifactorial and mostly is the result of “Pathologisation” (which we will talk about in a later post).
So having an x-ray, MRI or CT scan for your back pain will in most cases be a waste of your time and money. (The only exception to this rule is if you have signs or symptoms suggesting serious pathology like a fracture OR if you have constant pins and needles, numbness and weakness in a dermatomal distribution).
2. Disc bulges are more likely to cause leg symptoms rather than back pain. If you have back pain, and no leg symptoms, it is unlikely that a disc is the cause of your symptoms. The reason is that the disc itself is actually very poorly innervated (Garcia-Cosamalon and colleagues 2010) meaning that the disc itself does not contain a lot of sensory nerve fibres. It will really only start to cause you grief if it starts to contact and compress the nerve root. If it gets to this point, you may have pins and needles, numbness, weakness of the area supplied by the nerve that is affected. Even at this stage we can reliably diagnose it without the use of scans.
Patients with true disc bulge symptoms will most likely present to the clinic complaining of leg symptoms but no back pain.
3. Avoidance of movement can result in poorer outcomes . By all means avoid heavy lifting until your pain settles but there is no reason, nor any evidence, to suggest that avoiding bending or avoiding twisting will help healing or speed recovery. We actually know that stiff spines are painful spines so avoidance of specific movements can result in reduced mobility and reduced strength in the long term . Getting moving early, and recovering your mobility and flexibility early, with the help of a competent clinician, is the most effective treatment.
So if the above story sounds like you, don’t panic! Approximately 95% of patients with acute low back pain who present to a competent physiotherapist recover completely within 4 weeks, most even sooner.
If you’re reading this and have already had an MR or CT scan, remember these findings are normal and most likely are not the cause of your pain. Low back pain is multifactorial, so having it assessed by a competent practitioner is the fastest way to get you moving again.
Lower back pain is one of the most common musculoskeletal injuries or complaints with approximately 85% of people experiencing back pain at some point in their lives.
Disc bulges are also just as common, but not everyone experiences pain from a disc bulge. In fact up to 50% of people with disc bulges are asymptomatic (i.e. don’t get any symptoms). READ MORE ABOUT THIS IN OUR EARLIER ARTICLE HERE.
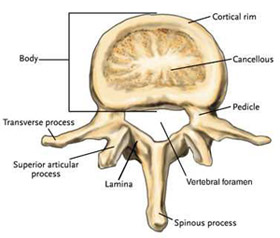
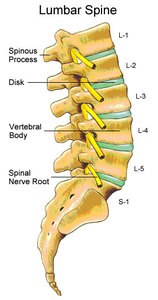
Lumbar Spine Anatomy
The lumbar spine consists of 5 lumbar vertebra and 5 corresponding nerve roots. The lumbar nerve roots exit the vertebra through spaces called foramen.
What happens when you do get symptoms from a disc bulge?
This is what is known in the medical world as "radiculopathy".
Radiculopathy is a pathological process where the nerve exiting the vertebra or the spine is being compressed. It can manifest in various signs including pins and needles, numbness, tingling, burning, nerve pain and weakness.
This can be due to changes in bony anatomy, degenerative changes or the dreaded bulging disc, which causes narrowing of the little gap where the nerve exits.
This little gap is called the nerve foramen and narrowing of the foramen is referred to as foraminal stenosis or nerve root impingement on MRI reports.
What exercises can i do if I have a bulging disc?
The short answer is lots!
There have been 2 fantastic studies done over the last 7 years which have proved that 2 activities that were thought to be bad for disc bulges are actually good!
Bending (lumbar flexion)
Running
1) Lumbar Flexion: Can I bend or should I keep my back straight?
In 2013, Singh and colleagues conducted Kinetic (dynamic) MRI’s on patients with disc bulges to assess for disc displacement as well as foraminal size which showed that lumbar flexion does not cause displacement of the discs, but actually increases the size of the foramen, which means more room for the nerve!
The take home messages from this study were:
A) Flexion (bending) showed a significant increase in foramen size on dynamic MRIs indicating an increase in size available for the exiting nerve root.
B) The amount of posterior disc bulge was significantly correlated with posterior movement into the foramen with extension not flexion. This indicates that there is greater compression of the nerve and increased posterior disc bulge when you move into extension (arch backwards) not flexion.
2) Running
Yes! You can do that too! A study published in 2017 by Belavy et al found those that ran 30-50kms/week actually had healthier, stronger, juicier lumbar discs compared to their less active counterparts.
What do I do if I have a disc bulge?
That’s Easy….Walk, run and DO NOT AVOID bending! The great news is that disc bulges do heal with time, with even the serious ones healing within 12 months.
There are lots of other options for exercise so if you’re not up to running or if you are have having trouble then please do not hesitate to get in touch with us at clinicalphysiostives.com.au
References
Singh V et al, Factors affecting dynamic foraminal stenosis in the lumbar spine, Spine J. (2013)
Belavý, D. L. et al. Running exercise strengthens the intervertebral disc. Sci. Rep. 7, 45975; doi: 10.1038/srep45975 (2017)