Ankle and Knee Stability and Landing Exercises
These are slightly more advanced exercises to perform after any ankle or knee injury for those wishing to return to sporting activities.
These are slightly more advanced exercises to perform after any ankle or knee injury for those wishing to return to sporting activities.
Medial Tibial Stress Syndrome (MTSS) or “shin splints” is one of the most commonly reported lower limb injuries by competitive and recreational athletes. Recent research has shown that shin splints affects approximately 20% of the running population, with the majority of sufferer’s partaking in long distance training/competition.
Currently, there is two widely accepted theories on the cause of shin splints:
The bony bending theory suggests that during running, the Tibia (shin bone) bends due to the stress placed upon it. This bending causes small amounts of strain in the bone that enables it to adapt and get stronger (a good thing!!). When this strain exceeds the adaption process the shin bone becomes overloaded (a bad thing!), subsequently leading to injury and pain.
The traction theory states that shins splints is caused by the continual contraction of the muscles (Soleus, Flexor Digitorum Longus & Tibialis Posterior) that attach to the inner border of the shin. As these muscles contract during running, they place a traction stress on the shin bone, which results in inflammation at their attachment onto the bone, causing pain.
Current research has identified several risk factors leading to an increased likelihood of developing shin splints. These include:
A previous history of shin splints
High Body Mass Index (BMI)
Female gender
Decreased running experience
Decreased running cadence (step rate)
Excessive pronation
Crossover running style
Increased vertical oscillation (ground clearance)
Forefoot running
To diagnose shin splints accurately, two symptoms must be present:
If you are experiencing symptoms not typical of shin splints such as cramping, pain spanning less than 5cm, burning pain, numbness or pins and needles, you should seek a thorough assessment by a physiotherapist to properly diagnose and treat your condition.
Arguably one of the biggest contributors to the development of shin splints in a runner is their running technique, particularly their lower limb mechanics. One of the quickest ways to reduce shin splints related pain is to address the technical aspects of running that can contribute to increased stress across the Tibia and associated musculature. What you should focus on is:
Increase your cadence!! – This is by far the biggest bang for your buck. Increasing your cadence by approximately 10%:
Reduces lower limb impact forces by 20%
Reduces ground contact time
Reduces stride length
The best way to achieve an increase in your cadence is by using GPS watches, phone applications or by simply running on a treadmill.
Eliminate a crossover running style – On a track, run straddling a line across 2 lanes or alternatively, try and maintain a space between your knees with every stride.
Strength exercises for shin splints should aim to improve the localised muscular capacity of the calf complex as well as the bone load capacity of the Tibia. This is best addressed with weight bearing functional exercises that mimic running postures.
One of the most important and often forgotten muscles of the calf complex is the Soleus. The soleus muscle is vital for absorbing excessive loads placed on the Tibia during running by minimising excessive pronation as well as resisting the bending forces experienced by the Tibia due to ground impact.
The best Soleus exercise that runners can do is the Bent Knee calf raise (pictured above). To perform the exercise correctly:
Bend your knee as far forward as possible, keeping your foot flat on the floor
Lower your heel back to the ground
Perform 3 sets of 15 repetitions in a slow and controlled manner.
As always, if you are having problems, please do not hesitate to contact one of our experienced physiotherapists.
About the authors.
Vas Krishnan is in his final year of Sports & Exercise Science at the University of Sydney.
Stephen Andreazza is a Titled Sports & Musculoskeletal Physiotherapist.
Lets face it, injuries are annoying and expensive. They result in lost hours of training and game time as well as dollars spent on physio, doctors and imaging, and in some cases, surgery. So what are the best ways to prevent injury? We highlight the key points taken from the most recent research as well as from Leicester City’s incredible Premier League Title in 2016.
Workload is all things affecting the body in a sporting context. This could be internal measures which are mainly physiological or external measures which are physical work performed. [8]
Internal Load Measures
External Load Measures
When quantifying workload for usable data we usually use at least one Internal load to determine intensity (e.g. RPE) and one external load to determine physical work done (e.g. Total Distance) these together help us to quantify total load (Internal load x external Load = total load).
It was found that using an internal load and an external load measure was more effective in determining the actual load an athlete was undertaking compared to just the external load. [8]
Calculating Load for a soccer player could be as simple as Minutes on ground x RPE. If a soccer player trained 3 times per week and had 1 game on the weekend where the sessions went for 60min each and their game time on game day was 60min. For Training sessions RPE was 6 and game day RPE was 8.
Session 1 – 60×6 = 360 Units
Session 2 – 60×6 = 360 Units
Session 3 – 60×6 = 360 Units
Game 1 – 60 x 8 = 480 Units
Total Weekly Load = 360+360+360+480 = 1560 Units
The Acute: Chronic Workload Ratio is a way for athletes and coaches to determine the load their athletes should do for current and future training as to prevent injury. If load is considered to be km running/week. Acute load is Km over 1 week and Chronic load Km over 4 weeks. [5]
Using the Acute: Chronic Workload Ratio we can quantify expected and required load for decreased injury risk. [5]
It was found that when the Acute: Chronic workload ratio was greater than 1.5 there was an increase in the risk of injury. This can be clearly seen in the graph below. [5]
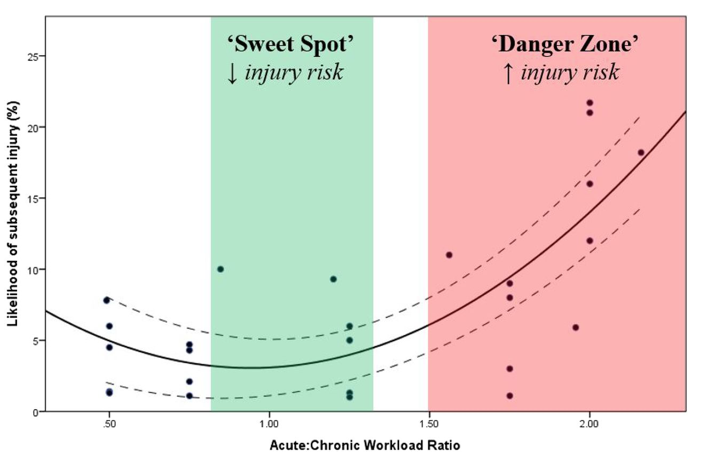
It was also found that >0.8 to <1.3 was the point of least injury risk. This was noted as the “sweet spot” and should be what all athletes are aiming to be in at all points of the season. [5]
>1.3 is where the risk of injury started to increase with a significant increase at 1.5 and an even greater increase at 2.0. [5]
Coaches and Athletes can use this as a guideline to determine the load that they should be using for transitioning season to season, coming back from injury or even coming back from holidays/time off. This can help the athlete and coach with injury prevention, re-injury and further progression. [5]
Below is a table illustrating what the likelihood of injury is for an athlete in accordance with the Acute:Chronic workload ratio. [1]
This table compares different scenarios of acute and chronic workloads using predefined equations to determine load as a percentage of normal training.[1]
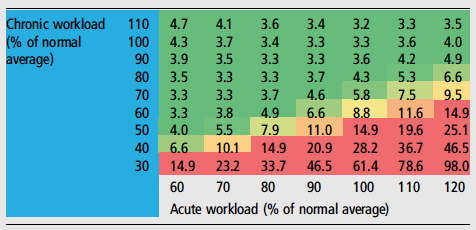
The table grades each load percentage with a percent likelihood of injury. [1]
For example if an athlete has come back from a holiday and resumed normal 100% load (Acute workload) but over the past 4 weeks has only been training at 30% of their normal load (Chronic Workload) there can be an expected 61.4% increased likelihood of injury in the following week. [1]
Athletes and coaches can use this table to determine the load they should be working at or if they are at a greater risk of injury. [1]
Acute: Chronic workload ratio should not exceed 1.3 or go below 0.8 (>0.8-<1.3) – aka “the sweet spot”
Likelihood of injury increases when the Acute: Chronic workload ratio is >1.3
Danger Zone for Injury when Acute: Chronic workload ratio is >1.5
Severe Danger Zone for injury when Acute: Chronic workload ration is >2.0 (greatest risk of injury)
The amount of “Load” that is too much is determined by how much you have been doing in the previous weeks.
An elite athlete training 6+ times per week will have a vastly different load to a high school athlete training 3 times per week, however we want their Acute: Chronic Workload Ratios to be the same!
Leicester City’s exercise scientists and coaches were meticulous about manage player loads. They used GPS tracking as one of a few tools to measure each players load.
If a player had spike in their workload, the coaches were notified and the player was pulled from the next session and sent for recovery work.
This sounds so simple but we see people get it wrong all the time.
Athletes or Individuals wanting to compete in particular events must ensure they are training specific to that event. For example if you wanted to run a half marathon, you need to run! You don’t need to be in the pool swimming or doing reps on the bike.
You can start by running small distances and build your way up to 21 km. Using the Acute: Chronic Workload ratio and increasing your distance/load by 10% per week you can safely build your load and compete in the half marathon at your best.
Leicester City were specific in their injury prevention programs. They identified that the most common injury was a hamstring strain and that these occurred in the last 20mins of a game when a player is trying to sprint under fatigue. They used 2 training methods to specifically address this.
https://www.valdperformance.com/nordbord-hamstring-testing-system/
At the end of the season, Leicester City had the least number of injuries in the league and also had the greatest number of counter attacking goals in the league. [7]
If all of this is still confusing to you (you’re probably not alone!) then at least try to stick to these simple guidelines.
If you’re still unsure, then please don’t hesitate to contact our friendly team at clinicalphysiostives.com.au
Drew et al. (2016)
Load Management is Critical for all types of Injury Prevention. This was found in relation to both specific pathologies/injuries and in controlling injury risk factors.
Murray et al. (2016)
Sudden increases in Acute workload were found to have a significant relation to injury in the current and subsequent weeks of increased load. High Chronic workloads were found to have a protective affect against injury. Hence the need for monitoring of both Acute and Chronic Load, and the Acute:Chronic Load Ratio.
Blanch et al. (2015)
“The Acute: Chronic Workload ratio should be included in the return to sport decision-making process” (1. p.475)
Concussion
With winter sport starting up again, it seems a perfect time to talk about concussion. Concussion seems to be the hot topic over the past few years. Sports commentators are talking about it far more than ever before. Even Hollywood has shown the impact of concussion on people’s lives.
In this article we will cover:
What is Concussion?
Signs and symptoms
What do the latest guidelines say about assessment and treatment
When can a player return to sport
Post concussion syndrome and how physio plays an integral role in rehabilitation
What is concussion?
Concussion is a head injury caused by traumatic forces to the brain. This can happen either by a direct hit to the head or a ricochet effect from a big impact.
What does concussion look like?
There are obvious and subtle signs that someone has sustained a concussion.
Obvious
– Loss of consciousness
– Slow to get up.
– Confusion/disorientation
– Blank look
– Balance, walking and coordination problems
– Memory Loss – you can ask them some simple questions like “What venue are we at today? What half is it?
Subtle
– Drowsiness
– Dizziness
– Light and noise sensitivity
– More emotional than normal
– Feeling foggy
– Headache
What do the latest 2021 guidelines say about concussion?
A player who has a suspected concussion must be removed from the game immediately and must not return under any circumstances.
There are a few important initial things to do with a player suffering a suspected concussion:
1) Monitor symptoms, particularly for any serious symptoms. You should call in ambulance immediately if player has any of the following signs or symptoms:
Neck pain or tenderness
Double vision
Weakness or tingling/burning in arms or legs
Severe or increasing headache
Seizure or convulsion
Loss of consciousness
Deteriorating conscious state
Vomiting
Increasingly restless, agitated or combative
2) Player must not be left alone for 1-2 hours
3) Player must avoid alcohol
4) Player must not drive home, a responsible adult must drive them home.
5) You can conduct a memory test.
Within 72 hours of the initial injury, the player must be referred to an emergency department or see a medical professional who is experienced in concussion management.
Once the player has returned home, they need 24 hours of total rest from mental and physical activity. This includes minimal screen time, no school/work and no physical activity. The total minimum time for complete and relative rest (until symptoms had stopped with no medication) is 7 days for 19years and over and 14 days for 18years and under.
When can the player return to sport?
This time will vary from player to player however the minimum times are as follows:
– Under 18 years cannot return for at least 19 days after all symptoms have disappeared
– Over 18 years cannot return for at least 12 days after all symptoms have disappeared
Does headgear reduce the risk of concussion?
There is a strongly held idea that wearing headgear will reduce the risk of concussion. Significant research has been conducted in the area and unfortunately has not found that wearing headgear will reduce concussion risk. Does this mean you shouldn’t wear headgear…no! Headgear is particularly useful at reducing the risk of cut to the head, as well as the dreaded cauliflower ears.
How can physio help in concussion?
While most people will recover without problem from concussion, some players will develop post concussion syndrome (PCS). PCS can limit players from return to sport for extended periods of time.
Physiotherapy plays a key role in PCS and can help players to return to sport up 4 times quicker. Neck pain, stiffness, weakness and reduced joint position sense (JPE) all contribute to PCS and can be addressed with specific exercises and manual therapy.
If there is 1 key thing to remember with regards to concussion, it is this… “If in doubt, sit it out!”
If you have any questions regarding concussion or post concussion syndrome, please do not hesitate to get in touch with us.
Resources:
https://www.healthdirect.gov.au/concussion
Although stretching has long been promoted as an injury prevention method, recent systematic reviews conclude that there is no evidence to support its efficacy.
Static stretching involves moving the muscle or joint into an elongated position and holding the position for an extended period.
Historically, this type of stretching has been used to prepare the muscle for exercise.
Dynamic or ballistic stretching is when the muscles and joints are taken through their range of motion during movement. This type of practice is more specific to preparation for exercise and sports in particular
During the rehabilitation process care should be taken to not ‘bounce’ the muscle that is recovering from injury
Dynamic stretches have been shown to significantly increase tendon flexibility and elasticity and have been promoted for end-stage rehabilitation for tendon injuries
However, ballistic stretching involves eccentric contractions during the stretch phase, which may results in soreness or injury and therefore care should be taken when incorporating such stretches
Static stretching changes the muscle-tendon functions (range of motion and maximum voluntary contraction), which are related to mechanical changes of the muscle but not the actual tendon structure
In a 2019 study there was a decrease in muscle-tendon stiffness after static stretching observed immediately, but not 5 or 10min after stretching
Warm-ups are typically composed of a submaximal aerobic activity, stretching and a sport-specific activity
The stretching portion traditionally incorporated static stretching
However, there are numerous of studies demonstrating static stretching induced performance impairments
A number of researches have concluded that stretching has no effect on injury prevention (Gleim and McHugh 1997; Herbert and Gabriel 2002; Small et al. 2008).
Sustained static stretching can impair subsequent performance;
Maximal voluntary contraction
Isometric force and isokinetic torque
Training-related strength measures such as one repetition maximum lifts
Power-related performance measured such as vertical jump (jump height)
Sprints running economy (reaction, movement time and balance)
Agility
The acute negative effects of stretching seem to be associated with stretches at a duration of 60 seconds, while stretches of shorter duration may have less significant deficits
The most powerful injury prevention tool available is strength training, at increasing loads over a 6-8 week period.
It is important to differentiate between pre-exercise stretching (where stretching does not appear to prevent injury) and regular stretching outside periods of exercise (where there is some clinical and basic science evidence suggesting stretching may prevent injury)
Additionally, stretching does not seem to reduce the effects of DOMS (Delayed onset of Muscle Soreness)
Dynamic stretching which involves controlled movement through the active range of motion should be the choice pre-exercise.
Athletes often stretch after exercise in an attempt to improve range of motion and reduce the perception of musculotendinous stiffness. While it is a regular component of post-exercise regimens, there is limited evidence of the effect of stretching on various aspects of recovery
Lund et al. suggested that stretching following bouts of eccentric exercise may delay recovery. In a study investigating the effect of static stretching on DOMS following eccentric quadriceps of seven untrained females, they reported that recovery of strength was impaired in the group who stretched their quadriceps for three repetitions of 30 seconds each day after exercise caused further mechanical disruption and exacerbated muscle damage
In contrast, Torres et al. reported no effect of daily stretching on maximum voluntary contraction of the quadriceps following eccentric exercise in healthy untrained men .
Barbosa, G., Trajano, G., Dantas, G., Silva, B., & Vieira, W. (2019). Chronic Effects of Static and Dynamic Stretching on Hamstrings Eccentric Strength and Functional Performance. Journal Of Strength And Conditioning Research, 1. doi: 10.1519/jsc.0000000000003080
Bertolaccini, A., da Silva, A., Teixeira, E., Schoenfeld, B., & de Salles Painelli, V. (2019). Does the Expectancy on the Static Stretching Effect Interfere With Strength-Endurance Performance?. Journal Of Strength And Conditioning Research, 1. doi: 10.1519/jsc.0000000000003168
Brukner, P., Khan, K., Clarsen, B., Cook, J., Cools, A., & Crossley, K. et al. (2017). Brukner & Khan’s clinical sports medicine. North Ryde, N.S.W.: McGraw-Hill Education (Australia).
Konrad, A., Reiner, M., Thaller, S., & Tilp, M. (2019). The time course of muscle-tendon properties and function responses of a five-minute static stretching exercise. European Journal Of Sport Science, 1-9. doi: 10.1080/17461391.2019.1580319
Smith, J., Washell, B., Aini, M., Brown, S., & Hall, M. (2019). Effects of Static Stretching and Foam Rolling on Ankle Dorsiflexion Range of Motion. Medicine & Science In Sports & Exercise, 1. doi: 10.1249/mss.0000000000001964
Su, H., Chang, N., Wu, W., Guo, L., & Chu, I. (2017). Acute Effects of Foam Rolling, Static Stretching, and Dynamic Stretching During Warm-ups on Muscular Flexibility and Strength in Young Adults. Journal Of Sport Rehabilitation, 26(6), 469-477. doi: 10.1123/jsr.2016-0102
Williams, M., Harveson, L., Melton, J., Delobel, A., & Puentedura, E. (2013). The Acute Effects of Upper Extremity Stretching on Throwing Velocity in Baseball Throwers. Journal Of Sports Medicine, 2013, 1-7. doi: 10.1155/2013/481490
With winter sport starting up again, it seems a perfect time to talk about concussion. Concussion seems to be the hot topic over the past few years: Sports commentators are talking about it far more than ever before and even Hollywood has shown the impact of concussion on people’s lives.