The latest update on Physio and Headache management.
Back in 2016 Andrew wrote a great blog article on the role of physio in assessing and treating headache. Well with the headache that was 2020 behind us, I thought I would start the new year with the latest information and research on how physio can help that pain in your head.
What are the common headaches that physios see?
There are 3 common headache types that physios generally see:
Cervicogenic
Tension
Migraine
Cervicogenic (headache coming from the neck) are generally one sided, will start with neck pain and progress to the head. You may also find neck stiffness and checking your blind spot whilst driving to be difficult.
A cervicogenic headache is essentially referred pain from the neck that, due to a miscommunication of the nerves that supply the head and neck, the pain is perceived in the head, rather than the true source in the neck.
The pathophysiological basis for the referred pain is a “convergence” of nerves. To try to put it simply, the nerves that supply the head come into close proximity to the nerves that supply the neck. As the nerves from the neck make there way into the brain to communicate the message of neck dysfunction, they “converge” with the nerves that are carrying messages from the head. The end result is that the brain thinks the message is coming from the head, rather than the neck.
Tension headaches feel like you’re wearing a swimming cap that’s a little too tight! It will feel like a tightening pain around your whole head. You may also have neck pain related to this headache.
Migraine headaches are commonly one sided and intensely painful. Most people say they either feel sick in the stomach or don’t like bright lights/sound. Some people will also get an aura (seeing bright lights and colour) before their pain comes on. Neck pain can occur with Migraine however is less common.
Signs that your headache may be coming from you neck
1) Neck stiffness
2) Your headache changes when your turn your head i.e may be worse when trying to turn your head in one direction
3) Tenderness of the upper cervical region. It may be sore and sensitive to push on the muscles and joints at the top of your neck.
Does posture affect headaches?
How many times have you heard or thought ‘Wow I’ve got bad posture’. Well, all your worrying may be for nothing. There has been some great research into posture and headache, which has found that people with headaches have many different postures.
There was not one posture that made people more likely to suffer from headache.
Additionally, other factors such as stress, lack of sleep and reduced physical activity have a much larger effect on developing headaches.
So, is there a good posture? The best evidence we have suggests that changing posture, rather than having one specific posture, is the best approach to take.
Can physio help your headache?
Short answer…yes! There has been lots of research into physio and headache, which shows that we can help reduce the intensity, frequency and duration of headache.
How do we do this?
Hands on treatment of the joints and muscles in the neck can be very helpful to reduce headache pain and stiffness. However, the effects of these treatments don’t always treat the common, underlying muscle problem.
A study on 52 women in 2019 in the Journal of Orthopaedic & Sports Physical Therapy found that “Women with migraine demonstrated decreased neck flexor and extensor muscle endurance compared to women without migraine.”
We have found that improving the endurance of the neck muscles helps to improve the ability to do simple things like…reading, texting or even just sitting/standing long periods.
De Quervain’s Tenosynovitis is a painful condition which affects the thumb muscles (Abductor Pollicis Longus and extensor Pollicis Brevis).
Commonly seen in females who are in the post-natal phase, it is caused by a rapid increase in load on the thumb muscles and tendons. This over-load is usually caused from repetitive feeding positions, lifting and holding of an new infant. It can also commonly occur in golfers.
Symptoms will include swelling and local tenderness over the tendons. It can also be a sudden sharp feeling, which is not ideal when holding a young child!
Diagnosis
It is diagnosed by conducting a simple test called the Finkelstein test. The tests involves bending your thumb across the palm of you hand and then bending your fingers over the thumb. The wrist is then bent toward your little finger. If this reproduces the same pain you experience, it is likely De Quervains syndrome.
A physiotherapist will also conduct some tests on the joints around the thumb and wrist to exclude them as a source of the symptoms.
Treatment
Successful treatment techniques include splinting/bracing of the wrist to off-load the thumb tendons, and then progressive weaning from the brace to reintroduce load in a monitored way.
Gradual strengthening of the tendon is highly important as increasing the tendons tolerance to load is the fundamental component of rehab. As with any tendon strength program, load needs to be slowly introduced as a sudden increase in strength exercises can easily overload and aggravate the tendon! If bracing is left on for too long the tendon will become weaker and hence when you remove the brace the pain will come back.
If you start treatment early, your symptoms should improve over the next 4-6 weeks. If your symptoms start during or after pregnancy your symptoms are likely to resolve once breast feeding has stopped.
Despite common belief, a corticosteroid injection is not the first line treatment. An injection should only be considered if bracing and physiotherapy has failed over a 4-6 week period.
TOP TIPS:
ICE for pain relief
BRACE to off-load the tendon
STRENGTH to increase the tendons tolerance to load (likely the reason the thumb was sore in the first place).
CORTISONE injection only after 6 weeks if the above fails.
If you have any questions or if you think you may have De Quervain’s then please do not hesitate to get in touch with us here.
Headaches affect up to 50% of the population at some stage in their lives. At least 20% of all headaches and migraines can be attributed to the neck and some studies show this number may be significantly higher.
What is a cervicogenic headache?
A cervicogenic headache is essentially referred pain from the neck that, due to a miscommunication of the nerves that supply the head and neck, the pain is perceived in the head, rather than the true source in the neck. The pathophysiological basis for the referred pain isa “convergence” of nerves. To try to put it simply, the nerves that supply the head come into close proximity to the nerves that supply the neck. As the nerves from the neck make there way into the brain to communicate the message of neck dysfunction, they “converge” with the nerves that are carrying messages from the head and thus the end result is that the brain thinks the message is coming from the head, rather than the neck.
What can a physiotherapist do?
Our jobs, as physiotherapists, are to:
correctly identify headaches that are caused by a neck (cervical) dysfunction;
correctly identify what type of dysfunction it is and;
treat the underlying cause of the dysfunction to promote good, long-term outcomes.
How can we correctly identify a cervicogenic headache?
It can take 60-90mins to thoroughly assess and diagnose a headache as the symptoms and physical findings are complex and differ from patient to patient. The first step is to look at the history and symptoms. These typically include:
Gradual onset of symptoms (won’t come on sharply or suddenly)
Episodes are similar to each other i.e. symptoms do not worsen episode to episode
Location
Will generally by one-sided and will not shift sides within the same episode
Can be one of, or a combination of, neck, occipital (at the back), parietal (at the side) or orbital (around and behind the eye)
Can last anywhere from 1 hour to 1 week
Feels non-throbbing
Aggravated by neck movements or sustained postures
Other symptoms can include nausea, vomiting, visual disturbances and sensitivity to light and sound
If your symptoms fit the above criteria then the next step is to conduct a thorough musculoskeletal exam. This includes, but is not limited to,
Posture assessment
Ergonomic assessment if work seems to be an aggravating factor
Neck range of motion and strength testing
Shoulder and scapular range of motion
Thoracic range of motion
Palpation assessment, particularly looking for stiffness, position, tenderness and/or referred pain from the top 3 cervical joints
Cervical flexion rotation test (CFRT)
This test has been found to have good reliability in diagnosing cervicogenic headache (Hall et al, 2008)
If your symptoms still fit the criteria for a cervicogenic headache, we can then move on to addressing the findings from the physical assessment.
Treatment
Treatment will depend on the findings from the subjective history as well as the physical exam and can include, but are not limited to,
Neck and thoracic spine mobilisations
Thoracic manipulations
Ergonomic adjustments to workstation
Strengthening exercises for the deep neck stabilisers, neck and thoracic extensors and upper trapezius/shoulder girdle muscles.
Sustained Natural Apophyseal glides (SNAGs) for the C0- or C1-2segments (see video)
2 recent systematic reviews released in The European Spine Journal (Varatharajan et al, 2016) and the Journal of Manual Therapy (Gross et al 2016) both found that exercise combined with mobilisations is an effective treatment option for headache and can also decrease medication intake in the short and long term.
If the above signs and symptoms sound familiar, then please do yourself a favour and book an appointment with an experienced physiotherapist.
We show you the best 3 hamstring exercises to improve strength, speed and prevent injury.
In our latest video, Jin Su Jung, one of Australia’s top sprinters with a PB of 10.27, demonstrates our top 3 hamstring exercises to develop strength, speed and most importantly, prevent injury.
The most important thing to remember when prescribing hamstring exercises is that the exercise should mimic, as closely as possible, the actions, loads and positions that hamstrings go through, particularly at the point in the gait cycle that they tend to tear. This point is when the hamstring quickly moves from an eccentric (lengthening phase) to a concentric (shortening phase) which happens when the hip is flexed out in front and the knee moves from extension (straightening) to flexion (bending). If the hamstring is not strong enough to make the transition quickly, it will fail and “tear”.
The exercises
Do 3- 4 sets of 6-8 reps of each, twice a week. Try to NOT do it 24 hours PRIOR to a high intensity running/sprint session. Try to make the transitions from lengthening to shortening as quickly as possible and in a PAIN FREE manner.
Exercise no.1 – Nordic hamstring curl
Not my favourite as it is a double leg exercise and hamstring injuries are a single leg injury, however, it is the only single exercise thus far that has been proven, in 2 different studies, to reduce hamstring injury rates (Van der Horst et al 2015 & Peterson et al 2011).
Tips: Don’t “drop” at the end of the movement. If you are not strong enough to go all the way down then stop when you feel you are about to fail and pull back. Try to go a little lower each week.
Exercise no.2 – Single leg glute/ham raise on GHD machine
Tip: Keep the knee flexed (don’t let it straighten) the entire time and try to produce the movement through your hip/glute. MUST BE DONE AS A SINGLE LEG EXERCISE.
Exercise no.3 – Single leg skateboard hamstring curl/glute raise
Tip: Again do not let the knee straighten all the way. Skateboards are available at Kmart for about $30. Well worth it!
If you have had a hamstring tear then approach these exercises slowly. There are many other factors that can contribute to hamstring tears so if you do get recurrent hamstring tears or pain then please book yourself in to see an experienced musculoskeletal physiotherapist.
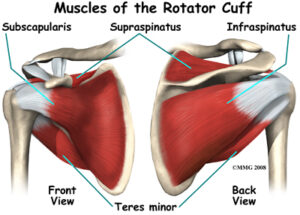
The important stuff you need to know about rotator cuff injuries.
The rotator cuff is a very important group of four small muscles (supraspinatus, infraspinatus, subscapularis & teres minor) that connect the upper arm to the shoulder blade (see image). Their main role is to not only move and control movements of your shoulder but to also provide dynamic stability to the shoulder joint.
Unfortunately, rotator cuff tears, which can occur to any one of these muscles, are one of the most common causes of shoulder pain and disability in both the sporting and general populations and can make everyday tasks increasingly difficult and often very painful.
Research has shown that the risk of developing a rotator cuff tear increases with age. Jobs and sports that require repetitive overhead work also increase the risk of rotator cuff injury. Jobs such as construction, carpentry, electricians and painters as well as sports that require overhead movements such as swimming, baseball, cricket and volleyball can all predispose the shoulder to injury.
How do rotator cuff tears occur?
Rotator cuff tears generally develop as a result of either:
Traumatic events – Such as a fall onto an outstretched arm or lifting a heavy object
Non- traumatic events – Such as excessive repetitive use or normal age related wear and tear
How do I know if I have a rotator cuff tear?
Symptoms of a rotator cuff tear can vary from person to person, however, common findings include:
Pain on the side or back of the shoulder
Pain in the upper arm.
Reduced shoulder movement and pain associated with overhead tasks such as changing a lightbulb or reaching for the top shelf of a kitchen cabinet or other tasks such as reaching behind your back or out to the side.
A feeling of weakness with shoulder movements
Pain sleeping on the affected side
Should I get a scan?
Imaging studies, both Ultrasound and MRI, have shown that the prevalence of rotator cuff tears in asymptomatic (symptom free) individuals is approximately 50% in those aged between 40 to 60 years of age, and as high as 80% in those older than 80 years of age. (Harris et al, 2012). This means that if a tear is present on an ultrasound or MRI it may just be due to the natural ageing process and not related to your shoulder symptoms at all.
If you have shoulder pain and are unsure whether you require imaging, your physiotherapist will be able to determine if your pain is caused by the presence of a tear or any other underlying factors.
How can physiotherapy help?
Research has shown that physiotherapy management, specifically strength training, should by the first treatment option for rotator cuff injuries (Ladermann et al, 2015; Ainsworth et al, 2007; Collin et al, 2015).
Rotator cuff tears account for over 50% of all shoulder conditions seen by physiotherapists on a regular basis (Donatelli, 2011).
The first thing that we will determine is whether your symptoms are in fact due to a tear to the rotator cuff. This is achieved by a thorough assessment of your shoulder, neck and upper back including:
A detailed history of your injury
Clinical examination of your shoulder movements and strength
Special orthopaedic shoulder tests
Examination of your neck and upper back movements
Palpation of your shoulder muscles and surrounding structures
Determine if imaging is required
Determine if you need to see an orthopaedic specialist
Set specific, individualised rehabilitation goal
What does treatment entail?
A 1 hour initial consultation is recommended for your first session. After your assessment, treatment may include:
Treatment and advice for pain reduction
Hands-on manual therapy for restoration of normal shoulder movement
Restoration of normal neck and upper back movement