Exercises for wrist and elbow pain
Try these beauties to improve pain around the wrist or elbow.
When doing the exercises, ensure you are not using the momentum of your body to help lift the weight.
Try these beauties to improve pain around the wrist or elbow.
When doing the exercises, ensure you are not using the momentum of your body to help lift the weight.
Three different exercises targeting the 3 different heads of the deltoids to give your shoulders a well-rounded workout!
When picking what exercise to do, choose one that is CHALLENGING for your balance. If it’s too easy, you won’t get better!
Balance training is important for elderly people to prevent falls and also for people with acute lower limb injuries such as an ankle sprain.
The term X-factor is used to describe the rotation of the shoulders in relation to the hip. Recent research (Myers 2008, Gordon 2009, Cheetham 2011 and Meister 2011) has found that there is a significant correlation between upper torso and pelvic separation and club head speed. In other words, the ability to rotate the upper trunk whilst keeping the pelvis still and vice versa. This separation utilises the muscle stretch shortening shortening cycle (SSC). The SSC explains the rapid change from an eccentric muscle contraction (when a muscle is lengthening) to a concentric contraction (when a muscle is shortening). This is a powerful tool inherent to all our muscles and is the reason why you can jump higher with a bit of a run up compared to just standing on the spot and jumping.
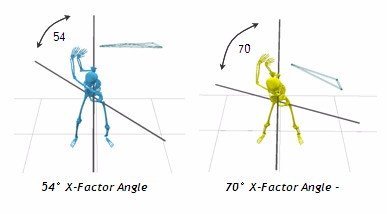
To utilise the natural SSC, the trunk muscles that produce rotation need to be on stretch at the top of the swing. The muscles we are talking about are the obliques, and some of the erector spinae muscle group that run up either side of your spine. To place the muscles on stretch, the upper trunk/thoracic spine needs to move independently of the pelvis.
But BEWARE… Your rotation should be produced predominantly from your thoracic spine , NOT your lumbar spine. There is only 5-20degrees of available rotation in the lumbar spine but 60-80 degrees in the thoracic spine. Low back pain in golfers has been linked to a lack of thoracic rotation which results in the body trying to gain rotation out of the lumbar spine.
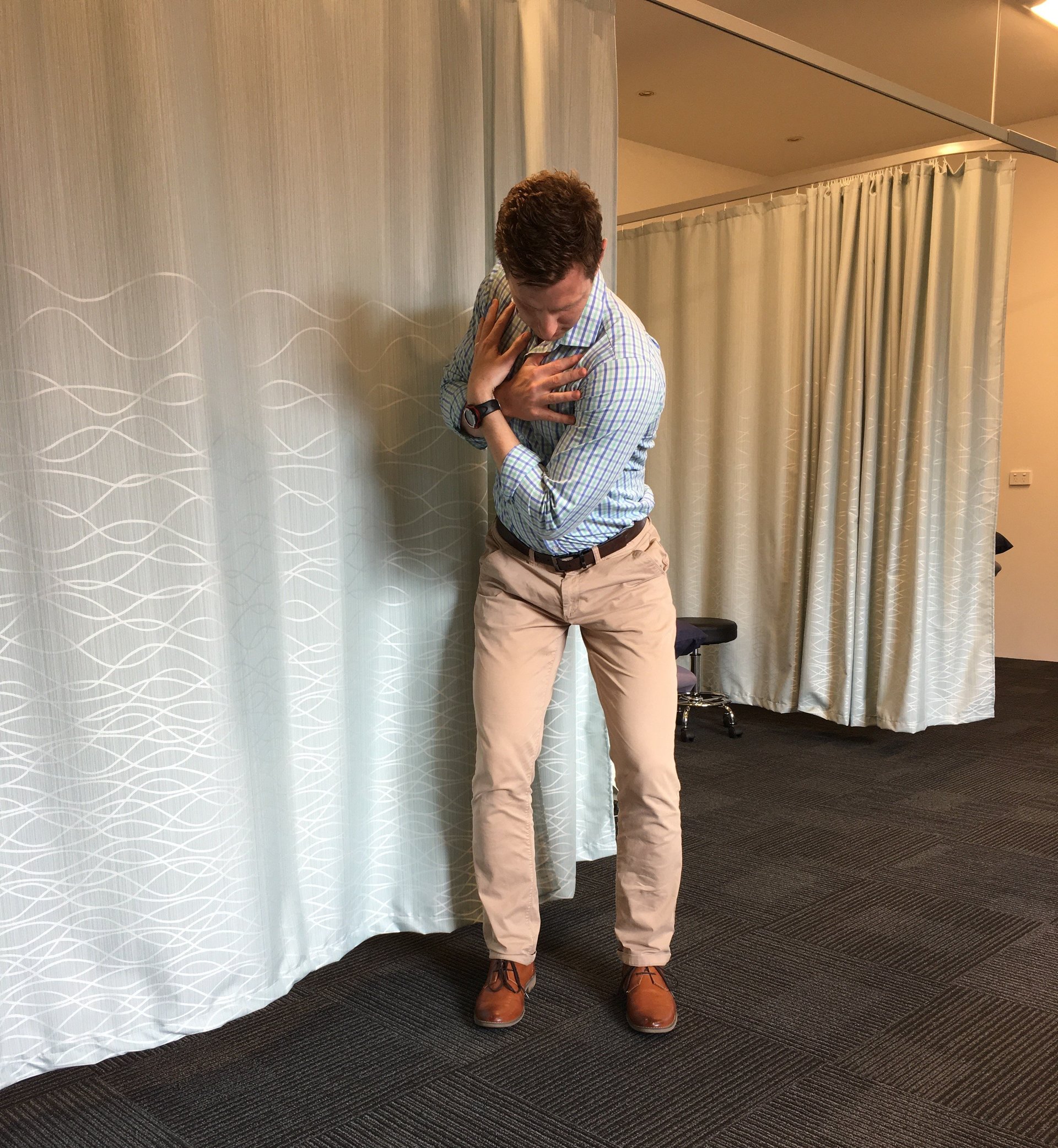
Try this simple drill. Stand in your golf stance, with hands across your chest. Keep you hips pointing straight ahead and try to rotate your shoulders/upper body to the right whilst maintaining your hip and pelvis position. You should almost be able to look over your left shoulder.
X-Factor Test
For a right-hander, lie on your left side with hips flexed to 90 degrees, knees together and arms outstretched. Keep your knees together, pelvis still and rotate your top arm up and over as far as you can. Aim to get your right shoulder blade on the floor. Perform 2 sets of 15 every day AND as part of your warm up.
For a right-hander, stand in your swing stance with the band attached at chest level to your left. Grip with both hands, keep arms straight and rotate trunk around to right, keeping hips and pelvis pointing straight ahead. Perform 3 sets of 10 once/day. As you improve you can step out further to increase resistance and also try standing on a 45 degree angle towards the band i.e. feet and hips pointing to the left 45 degrees.
There are a number of exercises that can be prescribed to address a lack of thoracic rotation including both mobility and strength exercises. if you would like to know more about how you can test and train the musculoskeletal system to get more out of your golf swing then please do not hesitate to contact us at our St Ives clinic at clinicalphysiostives.com.au
As a women’s health physiotherapist I frequently get asked about what type of exercise to do, how much to do, what is safe and how to return to exercise in pregnancy and postnatal period.
Below you can find all the evidence-based answers to the commonly asked questions that I get!
The current 2016 RANZC exercise during pregnancy guidelines recommend that pregnant women should aim to be physically active, preferably all days of the week and should accumulate between 150-300 minutes of moderate intensity exercise per week. Exercise should be at least 30 mins at a time but it is advised to limit duration to 60 mins, unless the exercise is at a light intensity.
We encourage women to begin some type of exercise during pregnancy, even if you have not exercised prior to pregnancy. We would recommend if you are just starting out, to have guidance from a women’s health physiotherapist and to gradually build up over time. If you have already been exercising it can be a good idea to check that your current program is appropriate.
Exercise intensity will depend on your baseline level of fitness and previous exercise routine. For those who have been previously inactive and are starting a new exercise program, maintaining a moderate level of intensity is recommended.
There is currently no evidence to suggest that women who previously participated in regular high intensity exercise and who continue to participate in vigorous exercise, are doing harm during pregnancy. Provided that they adjust the routine based on changes in comfort and tolerance.
Athletes should be wary of excessive exertion as fetal well-being may be compromised above a certain threshold of activity.
The talk test is quick and easy way to gauge exercise intensity. Intensity is considered moderate if you can comfortably hold a conversation, or is considered vigorous intensity if you have a need to pause for breath during conversation.
There isn’t a one type fits all approach to exercise, find an exercise that incorporates strength, flexibility and aerobic components, and most of all you should enjoy doing it!
Provided that there are no contraindications to exercise, pregnant women should participate in both aerobic and resistance based activity. Women should aim for two sessions of strengthening per week, on non-consecutive days. Resistance can be light weights, rubber bands or body weight and should be performed at a moderate intensity, slowly with appropriate breathing.
Some great forms of exercise when pregnant are:
Clinical Pilates: it is a great way to perform resistance exercise, and is tailored to the individual.
Walking is a good aerobic exercise but should be performed at a brisk pace.
Hydrotherapy is great in the later stages of pregnancy, especially for its weight supported nature. It also reduces lower limb swelling and oedema due to the redistribution of fluid. Prolonged immersion in waters above 34 should be avoided, and immersion at above this temperature during the first trimester is not advised.
Stationary bike/ Cycling
Swimming
Pregnancy yoga
Strength based gym classes.
Why we haven’t mentioned running and high impact exercises? You can participate in these activities if you were doing it regularly prior to pregnancy, however pregnancy is such a short time of a woman’s life, that avoiding high impact activity during this time when your body is experiencing ligament laxity and softening is a good idea. This can help to prevent incontinence and prolapse issues!
Heavy lifting
Hot yoga
Skydiving/ bungee jumping
Scuba diving
Activities with a high risk of falling or getting hit in the stomach
Activities that involve straining, holding the breath or
Working at a high and unaccustomed intensity
I would highly recommend at your next GP, midwife or Obstetrician review to ask if there are any medical issues that would affect your participation in exercise. As there are some conditions where exercise is not advised.
A number of changes will take place during pregnancy. Women will generally experience 10-15kg of weight gain to account for the baby, the placenta, amniotic fluid and increase in blood volume.
Vascular changes will occur especially in the second and third trimesters, where the cardiac volume will increase by 70-80mls, the cardiac output will increase by 40%,the resting heart rate will increase and blood pressure will decrease. These vascular changes reach maximum around the 20-24 weeks.
With this in mind, rapid postural changes should be avoided, heat and hydration levels should be closely monitored and women should be aware of how to track their level of exertion. It is advised to perform a cool down after exercise and not to stop suddenly.
Relaxin is a hormone that is commonly blamed for SIJ pain (also known as pelvic girdle pain) and ligament laxity during pregnancy. It is a hormone that prepares the lining of the uterus for the implantation of the embryo. Relaxin peaks at the 12th week and will stabilise to 50% of this level at 17 weeks. The Relaxin level will return to normal within hours to days of birth. However what we know is that joint laxity increases during pregnancy and is most marked in the last three months of pregnancy and 3 weeks postpartum (i.e Joint laxity increases even though relaxin levels stabilise at 17weeks).
Peripheral joint laxity does not return to normal ranges within the first 6 weeks post birth, therefore is advised to not participate in heavy joint loading exercises during these periods, such as jumping and changing direction.Women who have abnormally high levels of relaxin have been correlated to experience more pelvic girdle pain.
As the uterus grows with pregnancy, the weight of the enlarged uterus may abstract venous/ blood return. Therefore pregnant women in the second and third trimester should avoid exercise lying on the back for prolonged periods of time. Try sitting or standing instead.
Those who experience light-headaches, nausea or feel unwell when they exercise flat on their back should modify their exercise.
Activities that involve jumping or bouncing may add extra load to the pelvic floor muscles and connective tissue and are best avoided. Pelvic floor Strengthening exercises are generally recommended.
Exercise is now acknowledged as an effective way to decrease insulin resistance and thus help control blood glucose levels. It can prevent gestational diabetes if performed throughout the entire pregnancy at least three times per week.
Women should eat about 1 hour prior to exercise, to help balance blood glucose levels.
A general practitioner and/ or obstetrician will advise you if you have any contraindications to exercise. Examples of these may include cardiovascular disease, poorly controlled asthma, poorly controlled diabetes and bone or joint problems. They will also advise you if you have a pregnancy related complications.
Expectant mothers must be conscious of pregnancy-related complications, such as bleeding, sudden swelling, abdominal and back pains or decreased fetal movements. At the onset of any of these, activity should be ceased and seek medical assistance.
Back pain affects between 48-90 % of pregnant women. The most common locations are the sacroiliac joint at the back, and the pubic symphysis joint at the front. The lumbar spine and thoracic spine can also become painful however are generally less affected. Pregnancy-related Pelvic girdle pain is mostly likely to present between 18-22 weeks.
Generally low back pain that is present before pregnancy will start to feel better as pregnancy progresses, but new onset back pain during pregnancy may progressively increase if not managed appropriately. In pelvic girdle pain, resistance exercises are generally prescribed to increase the strength and endurance of pelvic stabilising muscles, such as the gluteal muscles.
The pelvic floor is a sling like structure of muscles, ligaments and connective tissue (fascia) that supports and contracts to hold the internal and reproductive organs up high and enables voluntary control of the bowel’s and urine.
Most women will benefit from doing pelvic floor exercises, not only for strength purposes but also to prepare you to relax the muscles during labour. The research shows that if you do pelvic floor exercises throughout pregnancy you will be less likely to be incontinent in the postnatal period.
The internal pelvic floor muscles will therefore be less likely to tear and have trauma if you can relax them.
Some women have the opposite of a weak pelvic floor, they can be too tight and over active! These women should not aim to increase pelvic floor tone and strength but rather have a strong focus on relaxing and letting go.
Remember that during a vaginal delivery some pelvic floor muscles and connective tissue’s have to stretch up to 600x their normal length. This is a significant amount of trauma and quite a shock to the system. Therefore in the early days postpartum, slow gentle walking is advisable.
Hormones that are present due to breastfeeding, can continue to cause ligament laxity, therefore it may take up to a year before your ligament laxity is back to normal. I would advise to limit unnecessary bouncing, running and heavy joint loading activities if you are still breastfeeding.
For pelvic floor strengthening before seeing pelvic physio, you could start your rehab by doing one pelvic floor contraction per week postpartum
For example:
I encourage women to be assessed in private practice, two weeks post delivery. This is to ensure appropriate management is commenced, and to make the most of healing time frames and hormone changes. An abdominal separation check may only take 40 mins and management can include abdominal bracing, taping, progressive strengthening and tips to avoid overload.
Generally at 6 weeks once medically cleared by GP or Obstetrician, a women’s health pelvic floor physiotherapist can assess the internal muscles. These assessments are very important for specific strength training depending on your pelvic floor presentation. From here measurements can be done to see whether you are ready to return to running, weight lifting, over head weights, standing weight, kicking, boxing, jumping etc.
If you need to book in to see Jessica for an assessment, please click here
This blog is based on the 2016 Royal Australian and New Zealand College of Obstetricians and Gynaecologists current recommendation guidelines for exercise in pregnancy.
For a more comprehensive guide see:
Although stretching has long been promoted as an injury prevention method, recent systematic reviews conclude that there is no evidence to support its efficacy.
Static stretching involves moving the muscle or joint into an elongated position and holding the position for an extended period.
Historically, this type of stretching has been used to prepare the muscle for exercise.
Dynamic or ballistic stretching is when the muscles and joints are taken through their range of motion during movement. This type of practice is more specific to preparation for exercise and sports in particular
During the rehabilitation process care should be taken to not ‘bounce’ the muscle that is recovering from injury
Dynamic stretches have been shown to significantly increase tendon flexibility and elasticity and have been promoted for end-stage rehabilitation for tendon injuries
However, ballistic stretching involves eccentric contractions during the stretch phase, which may results in soreness or injury and therefore care should be taken when incorporating such stretches
Static stretching changes the muscle-tendon functions (range of motion and maximum voluntary contraction), which are related to mechanical changes of the muscle but not the actual tendon structure
In a 2019 study there was a decrease in muscle-tendon stiffness after static stretching observed immediately, but not 5 or 10min after stretching
Warm-ups are typically composed of a submaximal aerobic activity, stretching and a sport-specific activity
The stretching portion traditionally incorporated static stretching
However, there are numerous of studies demonstrating static stretching induced performance impairments
A number of researches have concluded that stretching has no effect on injury prevention (Gleim and McHugh 1997; Herbert and Gabriel 2002; Small et al. 2008).
Sustained static stretching can impair subsequent performance;
Maximal voluntary contraction
Isometric force and isokinetic torque
Training-related strength measures such as one repetition maximum lifts
Power-related performance measured such as vertical jump (jump height)
Sprints running economy (reaction, movement time and balance)
Agility
The acute negative effects of stretching seem to be associated with stretches at a duration of 60 seconds, while stretches of shorter duration may have less significant deficits
The most powerful injury prevention tool available is strength training, at increasing loads over a 6-8 week period.
It is important to differentiate between pre-exercise stretching (where stretching does not appear to prevent injury) and regular stretching outside periods of exercise (where there is some clinical and basic science evidence suggesting stretching may prevent injury)
Additionally, stretching does not seem to reduce the effects of DOMS (Delayed onset of Muscle Soreness)
Dynamic stretching which involves controlled movement through the active range of motion should be the choice pre-exercise.
Athletes often stretch after exercise in an attempt to improve range of motion and reduce the perception of musculotendinous stiffness. While it is a regular component of post-exercise regimens, there is limited evidence of the effect of stretching on various aspects of recovery
Lund et al. suggested that stretching following bouts of eccentric exercise may delay recovery. In a study investigating the effect of static stretching on DOMS following eccentric quadriceps of seven untrained females, they reported that recovery of strength was impaired in the group who stretched their quadriceps for three repetitions of 30 seconds each day after exercise caused further mechanical disruption and exacerbated muscle damage
In contrast, Torres et al. reported no effect of daily stretching on maximum voluntary contraction of the quadriceps following eccentric exercise in healthy untrained men .
Barbosa, G., Trajano, G., Dantas, G., Silva, B., & Vieira, W. (2019). Chronic Effects of Static and Dynamic Stretching on Hamstrings Eccentric Strength and Functional Performance. Journal Of Strength And Conditioning Research, 1. doi: 10.1519/jsc.0000000000003080
Bertolaccini, A., da Silva, A., Teixeira, E., Schoenfeld, B., & de Salles Painelli, V. (2019). Does the Expectancy on the Static Stretching Effect Interfere With Strength-Endurance Performance?. Journal Of Strength And Conditioning Research, 1. doi: 10.1519/jsc.0000000000003168
Brukner, P., Khan, K., Clarsen, B., Cook, J., Cools, A., & Crossley, K. et al. (2017). Brukner & Khan’s clinical sports medicine. North Ryde, N.S.W.: McGraw-Hill Education (Australia).
Konrad, A., Reiner, M., Thaller, S., & Tilp, M. (2019). The time course of muscle-tendon properties and function responses of a five-minute static stretching exercise. European Journal Of Sport Science, 1-9. doi: 10.1080/17461391.2019.1580319
Smith, J., Washell, B., Aini, M., Brown, S., & Hall, M. (2019). Effects of Static Stretching and Foam Rolling on Ankle Dorsiflexion Range of Motion. Medicine & Science In Sports & Exercise, 1. doi: 10.1249/mss.0000000000001964
Su, H., Chang, N., Wu, W., Guo, L., & Chu, I. (2017). Acute Effects of Foam Rolling, Static Stretching, and Dynamic Stretching During Warm-ups on Muscular Flexibility and Strength in Young Adults. Journal Of Sport Rehabilitation, 26(6), 469-477. doi: 10.1123/jsr.2016-0102
Williams, M., Harveson, L., Melton, J., Delobel, A., & Puentedura, E. (2013). The Acute Effects of Upper Extremity Stretching on Throwing Velocity in Baseball Throwers. Journal Of Sports Medicine, 2013, 1-7. doi: 10.1155/2013/481490